Health Communication In Southern Africa: Using Social Network Information to Design Effective Health Campaigns to Address HIV in Namibia
No Comments yet Abstract
Abstract
When programmers only use representative responses from target audiences, they may design an intervention that does not fit a community’s channel of communication. This study illustrates how to use social network analysis and community haracteristics to identify if communitywide health campaigns or mass media programmes best serve communities for communication interventions addressing HIV in Namibia. Interviews were conducted with Namibians from different households (N = 3763) in ten different communities over a year (October, 2003 to June, 2004). Based on community characteristics and social network analysis, group-based interventions rerecommended for seven of the ten communities, with varying suggestions for inclusion of critical groups and/or leaders within each area, and radio programmes to reach isolated groups. Additional suggestions for health interventions in each community are proposed from their community’s characteristics.
Introduction
When health campaign designers only use the average scores from a random sample of their target audience, they may design an intervention that does not fit the community’s channels of communication. When misfits occur, diffusion of information, norms, or behaviours may not occur or may generate unintended community activities, such as ostracism and stigmatisation. Information about the community’s social system – its groups and their interconnections – could allow designers to adjust their interventions to these social influences. Community-level variables differ significantly from individual-level variables. They focus on group and social processes of leadership, equity, and social norms instead of individuallevel behaviours, attitudes, and perceptions. This chapter shows community networks created through people’s participation in social groups, and presents a decision-making model for interventions based on the community’s network and characteristics.
These data come from Namibia. Namibia sits on the northwestern border of South Africa, and South Africa ruled it from 1946 until 1988. Although differences between the countries exist (e.g., population size: 2 million in Namibia versus 44 million in South Africa), their similar HIV prevalence rates for adults (19.6% for Namibia, 18.8% for South Africa, UNAIDS, 2006) make this exploration in Namibia a useful opportunity to further health communication development in Namibia and South Africa. The next section details more about networks and health campaigns followed by details about HIV in Namibia.
Social networks and health communication
Imagine that Sarah, who lives in a rural community in Africa, attends a church meeting where she listens to a dramatic production about HIV transmission, treatment, and care for those living with HIV (e.g., DramAidE, Mbuyazi, 2004). As she talks with other audience members after the show, they may share information about HIV, reinforce or change existing social norms about HIV, and disclose their intentions to help (or not) those living with HIV. After leaving the drama, Sarah may also talk to those who did not attend the drama about its content as well as how other audience members reacted to it.
Through this process, information and social norms diffuse within the community. A map of communication patterns – a social network – of this community ahead of time, might have revealed this church and Sarah as having powerful, central positions within the network. Their central positions could provide them with great potential to diffuse HIV information, norms, and innovations in this community. One way to think about networks is as a system of water pipes. The pipes are channels for communication – the communication is the water flowing through them. As more pipes exist within a community, communication may flow more quickly and easily through the community. People tapping into the water system at strategic places, such as where many pipes come together, may have better opportunities to access communication flowing in the system, stop communication from flowing further, or to put their own messages into the system.
Social networks, then, can be thought of as people tied to each other through one or more specific types of interdependency (e.g., familial, emotional, or economic). A social network is a map of the relationships between actors (e.g., people, groups, leaders, objects, or events); social network analysis investigates these relationships (Wasserman & Faust, 1994).
Groups and social networks
One reason this system perspective is so powerful is that social network analysis matches many theories used to design communication interventions. For example, in social cognitive theory, Bandura (1997) argues that people are motivated to learn about, and then to engage in, behaviours if they know about them and see others performing them. Both social cognitive theory and diffusion of innovations (Rogers, 2003) describe how media campaigns are mediated through social networks: People may learn of new behaviours through the media and then pass on this information to their interpersonal networks (Bandura, 2004; Rogers, 2003). While mass media provide information, communication in these interpersonal networks provides receivers with guidance and support to enact, maintain, or cease such actions (Bandura, 1997; 2004; Rogers, 2003).
Indeed, Fishbein (2000; Fishbein & Yzer, 2003) synthesised predominant theories of health behaviour research and suggested that one key determinant is “environmental constraints preventing behavioural performance” (Fishbein & Yzer, 2003, p. 166). Network analysis emphasises structural relationships as key explanatory concepts (Wasserman & Faust, 1994). It assumes that the structural properties of social formations are factors that shape the perceptions, beliefs, attitudes, and actions of individuals and groups. Thus, direct and indirect exchanges among social actors possessing differential resources (e.g., information, money, or power) may facilitate or constrain social influence and collective action. Individual community members, like Sarah, who take part in a social network would have greater social capital than people isolated from the community’s social network. Her social capital may allow her greater access to knowledge, support, and resources (Fullilove, Green, & Fullilove 2000; Putnam, 2000).
A social network analysis map may be tailored to show which community
members have inaccurate knowledge about a given health issue, and might show that these people cluster within an inter-connected set of social groups. Where significance testing from random sampling procedures may miss changes in the knowledge, attitudes, or behaviour of a small cluster of people (Cohen 1994; Gondolf, 2004), a programmer armed with a network analysis could strategically focus a health intervention towards a disadvantaged cluster. On the other hand, if the network analysis shows that inaccurate knowledge is spread throughout a community, then the programmer may design a community-wide intervention or a mass media campaign with the knowledge that it will be diffused through these social groups.
Group memberships
There is good reason to test if a community is ripe for a community-based programme as many of these programmes are successful (e.g., Farquhar, 1978;
Keating et al., 1985; Nutbeam & Catford, 1987; Puska et al., 1983), such as community-based and clinic-based interventions for cancer screening (Pasick et al., 2004). Community-based programmes work for many reasons. Learning health information in groups from trusted sources replicates existing cultural patterns within many communities. Finally, as people feel stronger connections to their social groups, they attribute more credibility to group members as sources of information (e.g., Weenig & Midden 1991), with source credibility improving persuasion (e.g., Cialdini, 2008).
Such programmes, however, do not fit all communities. A meta-analysis of community-based interventions shows that many interventions work somewhere, but not one intervention works everywhere (Pasick et al., 2004). Successful interventions match features of the community, the target audience, and the objective, as well as intervention resources. One basic criterion for a group-based intervention is to ascertain how many people within a community participate in a social group. In addition to this basic criterion, important community characteristics to index include receptivity to change, perceptions of people living with HIV and AIDS (PLHA), leadership, group cohesion, active minorities, and communication patterns (Kincaid, 2004; Rogers, 2003). Many of these variables may exist at the citizen or group-level. For example, active minorities may be members within a group or groups within a community.
As for leadership, in some communities, particular social groups have more power than others within the community’s social network. One way to understand how much power a particular social group holds within a community is to estimate its network centrality (Wasserman & Faust, 1994).
Centrality: Groups and leaders
If most people participate in one group, such as the Catholic Church, and take part in two or three additional groups, such as athletic clubs or performing groups, then the Catholic Church would be central in that community’s network of memberships. If you presented information to members of the Catholic Church, then its members could disseminate the information to all their other social groups. Leaders may also be central within a social network because they lead a central group or because they lead multiple groups. Using local leadership well can improve an intervention’s success. For example, one way to introduce information into a group is to train one member in health information. In comparing mass media and member-training interventions, Lam et al. (2003) found that both channels may improve people’s health knowledge, but evoking actions, such as testing, only appeared in member-training interventions. Lam et al. (2003) argued that these trained group members “are effective because they use their cultural knowledge and social networks to generate change” (p. 516). In another example, participation in a mercury discussion network in Brazil was positively correlated with awareness of the critical information needed to change dietary habits (Mertens et al., 2008). The researchers noted that a community collaborator held a central position within this discussion network, and credited some of the programme’s success to his placement within it. This system-level information, central groups and leaders, can be critical information to guide interventions aimed at the diffusion and adoption of complicated behaviours.
System-level information may not represent cultural or social expectations of leadership and decision-making. Respondents may see their own leader as the
reasonable person to select and to guide group mobilisation activities in most communities. If leaders are not involved in this process, the programmes may not be effective. On the other hand, if all members of a group are expected to be involved in decisions and activities that affect the entire group, then leader-driven interventions may be inappropriate and ineffective.
Intergroup and intragroup considerations
One design concern for group-based interventions is whether to plan group activities that would involve multiple groups working together in a community effort, or to have separate group activities. Some people may feel confident that their groups could mobilise resources effectively without working with other groups. Forcing them to work together in a community effort may be problematic because one must coordinate these different groups.
In addition, although many studies show positive outcomes of group-based interventions, some studies have shown the difficulties of engaging in a discussion about HIV/AIDS (e.g., Gruber & Caffrey, 2005). In such contexts, voluntary involvement and human resources dedicated to HIV/AIDS-focused activities may be constricted and contentious (Gruber & Caffrey, 2005).
People’s confidence in their ability to confront others with sensitive information predicts if a confrontation takes place or whether a person decides to keep quiet (Makoul & Roloff, 1998). Reported confidence in helping those living with HIV in spite of opposition from the family or community predicts desires to keep a family member’s HIV diagnosis a secret (Smith & Niedermyer, in press). In Namibia a stigma surrounding HIV/AIDS exists. For orphaned and vulnerable children in Namibia, children’s ability to secure support has been tied directly to their parents’ cause of death (e.g., Ruiz-Casares, 2006). Although non-profit organizations, such as Red Cross International, are concerned about the secrecy surrounding HIV, their efforts are focusing first on reducing the stigma and discrimination attached to HIV in Namibia (e.g., Tjaronda, 2004). With stigmatised issues, it may be critical to assess people’s confidence that they would help people living with HIV even if someone, such as a family member or spouse, opposed them helping.
In fragmented communities, programmers may have to use mass media channels to reach into the different social networks. Whereas people naturally transmit new information to each other interpersonally (Granovetter, 1973), in a fragmented community mass media channels may be needed to ensure that everyone receives information. Without care, information and resources sent into fragmented communities can generate community-level inequalities in information and social support (i.e., social capital, Fullilove, Green & Fullilove, 2000; Putnam, 2000). Information about interpersonal and mass media channels can help programmers select the best channel to reach isolated community members.
Namibia and HIV
Despite years of HIV campaigns and health education presence in Namibia, HIV/AIDS prevalence is still climbing (UNAIDS, 2006). Due in part to AIDSrelated deaths, Namibian life expectancy dropped from 61 years (1991) to 53 years (2006, UNAIDS, 2006). In Namibia, 85,000 children have been orphaned due to the AIDS-related deaths of one or both of their parents (UNAIDS, 2006). These orphaned and vulnerable children (OVCs) are in need of adoption, and yet, extended families and communities are often reluctant to take them in (WHO, 2002). Health educators are trying to understand why family and community members are not taking in these children and how to persuade communities to adopt them (UNAIDS, 2004, 2006).
With the epidemic generalised and still on an upward trajectory, the Namibian government and its partners, including the United States Agency for International Development (USAID), have committed to providing a full range of prevention, care, support and treatment programmes, for higher-risk groups, people living with HIV/AIDS, their families and the orphans and vulnerable children affected by the epidemic. Nevertheless, Namibia is a vast, culturally diverse country, with a widely dispersed and largely poor population, which may require a tailored, communitybased approach with strong policy, financial and implementation oversight.
Methods
Participants and procedures
Namibian households (N = 3763) immediately adjacent to ten hospitals located throughout the country were interviewed (approximately 375 respondents in each location). The data took a year to collect (October, 2003: Oshikuku, Oniipa, Rehoboth; June, 2004: Andara, Nyangana and Rundu; and October, 2004: Katutura, Keetmanshoop, Oshakati, and Walvis Bay, see Smith, Witte & Keulder, 2004 for more information). In each region, researchers drew fresh maps that listed all formal and informal households within a 10-kilometre area surrounding the mission hospital. Interviewers stopped at each household, spiralling out from the hospital, and spoke with one eligible household member who was selected at random. They continued stopping at households until they completed their set number of interviews.
Interviewers had to be fluent in English and Afrikaans, as well as other local languages. Enumerators approached each selected household and asked to talk to the head of the household or the oldest person in the home. A family member (aged 15 years and older and residing in the household) was chosen at random to be interviewed in a private place either inside or outside of the household. The enumerator read the informed consent information, which explained that participation was voluntary and their answers were confidential. At the end of the interview, the respondent was thanked with a household food item (e.g., small bag of rice or flour). The entire instrument contained questions assessing behaviours related to HIV prevention and care and support, psychosocial factors believed to influence these behaviours, perceptions of the community-level characteristics, and exposure to mass media and community-based messages related to HIV/AIDS, which appear elsewhere (Smith, Ferrara & Witte, 2007; Smith & Morrison, 2006; Smith & Nguyen, 2008).
Instrumentation
Group membership. Respondents were asked to name all the groups of which they held memberships. Respondents could name as many groups as they liked. These groups ranged from sporting clubs (e.g., Young Tswana football club), professional organizations (nurses’ union), and religious groups (e.g., St. John’s church choir). The respondents and their groups were entered into UCINET 6.0 for Windows spreadsheet (Borgatti, Everett & Freeman, 2002).
Most important group. After naming all of their social memberships, respondents were asked to name the group they regarded as most important to them. Respondents could only name one group for this category.
Leadership. Respondents were asked to name the leader of their most important group. Respondents could name as many people as they liked. The nominated leaders, participants, and the groups were entered into UCINET 6.0 for Windows spreadsheet (Borgatti, Everett & Freeman, 2002); this programme was used to calculate centrality and density scores.
Responsible for group decisions. Respondents were asked a single question of who should be responsible for making decisions that affected the entire group.
Participants could select from the following choices: leader, elected representatives, entire group, or do not know.
Information seeking about HIV/AIDS. Respondents were asked if they had ever discussed whether HIV can be passed from a mother to her child during a group meeting (1 = yes, 0 = no).
Group sources for HIV/AIDS information. Respondents were asked to name groups that they would turn to for advice or information about HIV/AIDS.
Respondents could name up to five different groups. If respondents freely answered that they would go to no other group for information, then this answer was recorded.
Non-group sources for HIV/AIDS information. Respondents were asked six questions about where they get most of their information on HIV/AIDS (1 = yes, 0 = no). Respondents could mark more than one source. These sources included teachers, church, government, newspaper, radio, and television.
Group activities. Respondents were asked two questions about the activities of their most important social group. Respondents were asked if their most important group mobilised resources to help people affected by HIV/AIDS (1 = strongly disagree; 4 = strongly agree). They were then asked if their group had done anything to help people in the community affected by HIV/AIDS (1 = yes, 0 = no).
Efficacy to resist opposition. Participants were asked three questions to index how confident they felt about their ability to help someone living with HIV if (a) their spouse opposed, (b) members of their most important social group opposed, and (c) if no one else was helping (1 = not at all confident; 4 = very confident). The items were averaged into a single score, α = .78.
Results
Group membership
Before designing group-based interventions for communities, one must first learn if people participate in social groups, and if so, in how many. Interviewers asked respondents in each location to name the social groups in which they participated. Most people (modal response) participated in a single group, except in Oniipa and Rundu where most people belonged to three different groups (see Table 1). In Oniipa and Rundu, many residents may be able to transmit information they learn in one group to another group.
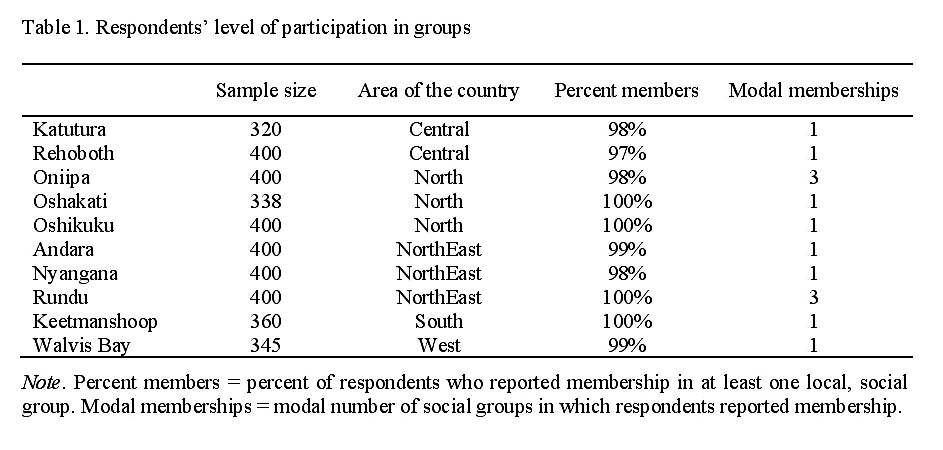
Table 1. Respondents’ level of participation in groups Note. Percent members = percent of respondents who reported membership in at least one local, social group. Modal memberships = modal number of social groups in which respondents reported membership.
In the other eight locations, residents may receive information in their group
meetings, but information moves less easily from group to group. Programmers would need to either (a) bring information to each group, or (b) see if the same people lead these social groups. If the same people lead multiple groups, then these leaders may transmit information from group to group, thereby diffusing information through the community.
Considering social groups
When many groups exist in a given community, it may become impractical to implement group-based intervention programmes (see Table 2). This situation
appeared in Katutura and Keetmanshoop where respondents named more social groups (232 and 213 groups, respectively) than at any other location (on average residents in other communities named 90 different social groups, SD = 31). Not surprisingly, fewer respondents in these two communities reported participation in any given group, in other words, any given group intervention would have direct contact with fewer people. Although group-based interventions may still be effective in communities with lots of social groups, it may be too costly to implement them.

Table 2. Group characteristics by catchments Note. ELCIN = Evangelical Lutheran Church in Namibia. RCC = Roman Catholic Church. CAA = Catholic AIDS Action. MTCT = Mother to child transmission of HIV.
Respondents also named their most important group, the group that influenced them the most. In most cases, popularity and influence co-existed, that is, the most popular groups were named most frequently as the most influential groups. This pattern appeared in each community except in Katutura. In Katutura, more residents said they were members of the Catholic Church than any other group, yet more residents said that the Evangelical Lutheran Church influenced them more than any other group. When the most popular groups are also seen as the most influential groups, then designers may strongly benefit from including these groups in grouptraining programmes from an early stage. On the other hand, when discrepancies between popularity and influence appear, designers may need to include both groups to tap into both communication and influence channels.
Centrality in membership network
One way to understand how much power a particular social group holds within a community is to estimate its network centrality (Wasserman & Faust 1994, see Table 3). The estimate of degree centrality for these locations varies from 95% in Nyangana to 5% in Oshakati (M = 44%). The high centrality score indicates that most respondents participate in one group, making it central.
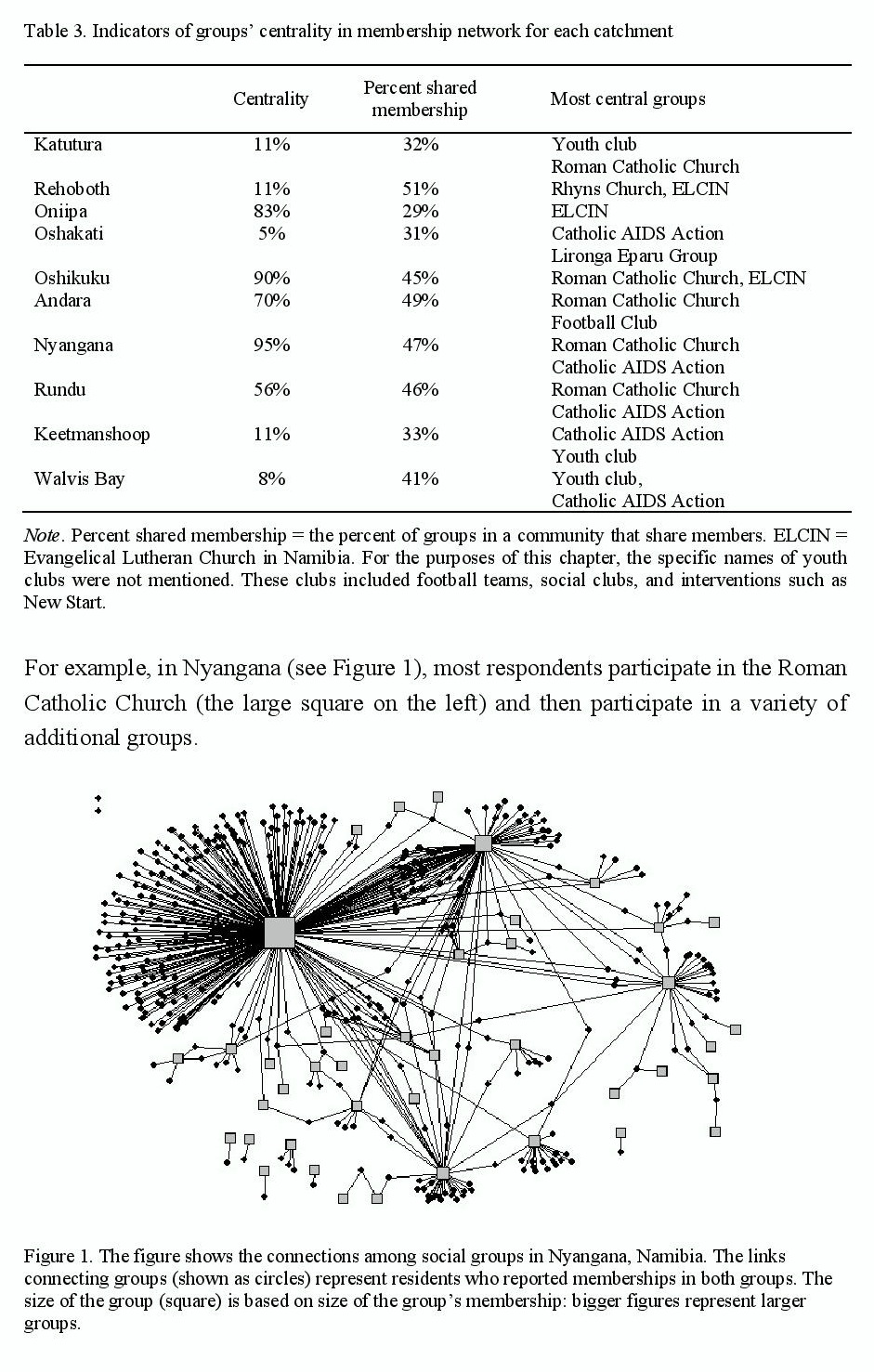
Table 3. Indicators of groups’ centrality in membership network for each catchment Note. Percent shared membership = the percent of groups in a community that share members. ELCIN = Evangelical Lutheran Church in Namibia. For the purposes of this chapter, the specific names of youth clubs were not mentioned. These clubs included football teams, social clubs, and interventions such as New Start. Figure 1. The figure shows the connections among social groups in Nyangana, Namibia. The links connecting groups (shown as circles) represent residents who reported memberships in both groups. The size of the group (square) is based on size of the group’s membership: bigger figures represent larger groups.
For example, in Nyangana (see Figure 1), most respondents participate in the Roman Catholic Church (the large square on the left) and then participate in a variety of additional groups.
Within Nyangana’s social network map of memberships the Roman Catholic Church is in a focal position, which suggests that it should be included in the campaign’s design. Oniipa, Oshikuku, and Nyangana have high centrality scores within their communities. This finding indicates that one group or a few groups hold privileged positions within these communities’ network.
Centrality in leadership network
Another way that information may move between social groups is through common leadership. One person may lead two or more social groups in a community and may distribute information and guidance among these groups. In general, the degree centrality scores for the leadership networks are low (from 8% to 22%, M = 12%) (see Table 4). This estimate indicates that very few leaders are central.
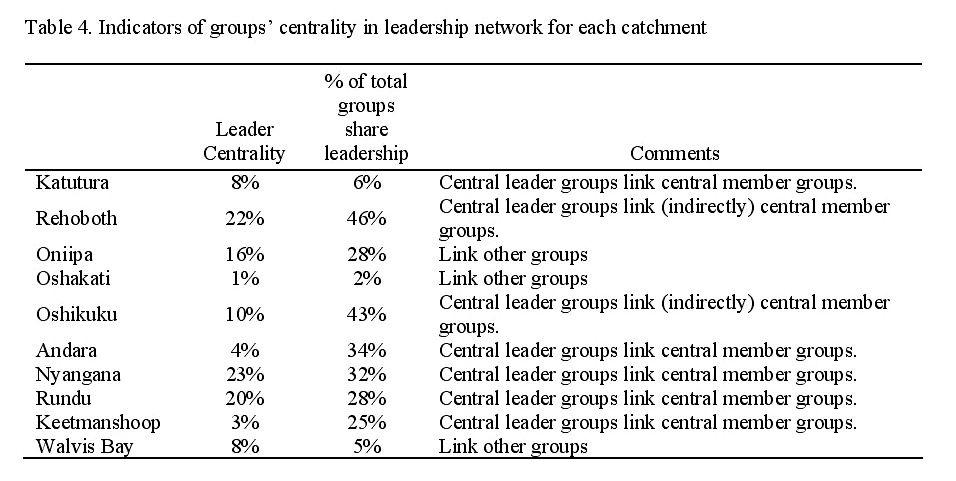
Table 4. Indicators of groups’ centrality in leadership network for each catchment
In addition, the three groups that are central in the network of leaders are also central in the network of members. Rehoboth shows the most connected network through leaders: 46% of the groups share leadership. Rehoboth’s leaders have more potential power over the communication flowing through the community and a greater reach to more groups. Within Nyangana’s network, two popular groups, the Roman Catholic Church and the Catholic AIDS Action, are connected through multiple leaders. Because they link two popular groups, these trained leaders could efficiently disseminate information to many sectors of the community. That said, only eleven groups are networked through shared leadership; which represents about 25% of all the social groups described in Nyangana. Interventions that rely exclusively on central leaders for dissemination may miss segments of the community.
Respondents were also asked to name the leader of their most important social group. The majority of respondents (M = 55%, SD = 16) showed consensus by
naming the same person as the leader of their group. The least amount of consensus appeared in Rehoboth and Oshikuku, where more than half of the respondents (85% and 57% respectively) either named different people as the leader of their group or could not name anyone as the group’s leader. Interestingly, these two areas also showed the most connected networks through shared leaders. Together, these two findings may indicate that although a few people lead many groups in Rehoboth and Oshikuku, these leaders do not hold dominant power within any group. These two communities may be good candidates for collaborative, multiple-group activities, leading to community-wide action.
Group decisions
Another consideration for programmes delivered within group meetings is whom people believe should make decisions for the group. With the exception of Oniipa, the majority of respondents (M = 75%, SD = 13) across the rest of the locations said that the leader, owner, or elected representative should make decisions that affect the whole group. In Oniipa, over half of the respondents (54%) felt that the whole group should be involved in such decisions.
Information seeking about HIV or AIDS
Before designing group-based interventions, it is helpful to know if people in these areas currently discuss HIV/AIDS within their groups or if such discussions would be new (see Table 2). Most respondents (70%, SD = 17) said that they talked about mother-to-child transmission of HIV (MTCT) in their group meeting. Across the locations about half of the respondents or fewer (53% to 17%) went to other groups for information. The most common source they listed, besides their own group, was the Catholic AIDS Action.
Top source for HIV/AIDS information
Some social groups are isolated from the membership and leadership networks in every location. Mass media programmes or community-wide programmes may be needed to reach these isolated groups. Across locations, respondents (M = 79%, SD = 11) said radio was the top source for information about HIV/AIDS, followed by other mass media sources, friends, and church. Most people (89%) own a radio, making radio programmes an excellent place to provide HIV/AIDS programming. This information could be compared with data gathered through the traditional, representative sampling before a final decision is reached.
Group activities and efficacy to resist opposition
Over half of the respondents (M = 64%, SD = 10) felt their groups could work independently and could mobilise resources for those affected by HIV/AIDS.
Interestingly, when asked, many of the respondents (50%) could not recall an action taken by their group to help those living with HIV.
Social pressure can mobilise or inhibit support for those living with HIV. Across communities, only 36% of respondents (SD = 13) were very confident that they would help someone living with HIV if they hit social opposition (if their spouse, social groups, or community opposed them helping those living with HIV).
Discussion
Programmers have choices for designing interventions. One option is to produce campaigns designed for delivery within or diffusion through existing social groups. Social groups provide people with a chance to discuss the presentations, to encourage each other to adopt new information, attitudes, or behaviour, and to allow information to diffuse to those who do not have access to the mass media campaigns (Bandura, 1997, 2004; Rogers, 2003). Group-based programmes have the best chance for quick diffusion if (a) the people participate in social groups, and (b) these groups are networked through shared members or shared leaders. The findings for the catchments in Namibia showed that group-based interventions fit seven of the ten communities well. Some community groups and leaders had powerful positions within the social network, making them important groups to consider when tailoring a campaign to a particular community.
Central groups
Central groups may critically shape their community’s dialogue and activities. For example, a central group could decide that certain topics are taboo, and then effectively shut down the information flow throughout the rest of the community. On the other hand, if groups share members, but no one group is central (low centrality scores), then information may flow through the community even if one group attempts to stop its dissemination.
Although it is important to discover groups’ centrality within the community’s network, it is just as important to discover which groups may exist outside of the network. Within every catchment, some groups were isolated from the community network. Programmers may need to target these groups separately, because information may not flow easily to them. In some communities, the respondents only participate in one group, so groups often do not share members. This leaves the community dialogue fragmented into many (often small), social groups.
Programmers would need to bring representatives from these many groups to a community information meeting in order for information to diffuse within the community – unless the groups share leaders who could diffuse the information from group to group.
The findings showed that in every location, except for Oshakati, the most popular group was a church; in Oshakati the group listed most frequently by respondents was the Catholic AIDS Action. Religious organizations play an important social role and their participation should be addressed in the interventions’ design. Special considerations may be necessary when disseminating messages in religious settings, because contextual information often guides how people determine the meaning of ambiguous words (Rodd, Gaskell & Marslen-Wilson, 2000). For example, a small study of youth, aged 15-25 in greater Windhoek Namibia showed that the youth confused the meaning of faithfulness as religious devotion instead of monogamy (Keulder & Witte, 2003).
Local leadership
When designing health interventions for distribution in social groups, the group’s leadership may be asked to pass on the information to its members. If respondents feel confidence in their leadership, then the leadership may be a useful source for distributing HIV information. In contrast, residents may feel more confidence in health care workers as sources for health information. In previous reports, respondents in different communities have shown different levels of confidence in their local leadership and their health care workers.
Although central leaders in a network analysis may have appeal because of their potential to distribute information quickly, these issues of trust and confidence should be included in decisions about who should start sharing HIV information in the community. In addition, the use of leadership should be considered in the context of who makes decisions within the community. In these findings, community leaders could guide in most of the catchments, but in Oniipa, the group members needed more direct involvement in promotion activities.
Understanding social resistance
The findings showed that the amount of residents who felt capable of resisting social opposition to working on HIV/AIDS-related issues varied between communities. Campaigns may first need to make social support for those living with HIV a norm before expecting residents to start providing support (UNAIDS, 2002). As stated by UNAIDS, Community mobilisation is the core strategy on which success against HIV has been built. Fostering such mobilisation requires eliminating stigma, developing partnerships between social and government actors, and systematically involving communities and individuals infected and affected by HIV/AIDS (2002, p. 16).
Gruber and Caffrey (2005) note that resource-poor countries, groups, and citizens may not be able to take on additional, challenging activities. “What is remarkable and inspiring is that so many communities have done just that” (p. 1217). The authors warn that although communities have shown remarkable collaboration, this response should not be presumed or taken for granted. Further, designers need to consider how interventions may exacerbate community inequities or may marginalise community members.
Two other considerations should be noted. HIV/AIDS prevention, treatment, and care are very different objectives for which very different approaches might be needed. Although previous studies document community-based interventions showing success with these three types of objectives (e.g., Rogers, 2003), the relationship between the objective and the norms, values, and goals of the local organizations is paramount. If the intervention’s objective and the organization’s mission do not align, the intervention can produce community conflict (e.g., Gruber & Caffrey, 2005).
Practical implications
If a community seems open to group programmes, one can evaluate if a couple of groups or a couple of leaders are more central within the area. Programmers should know to whom people attribute authority to take group decisions. This information can help ensure that certain groups or people are included within the programme development and implementation. This implication also means that community-level information may not generalise from community to community. Where principles of centrality, diffusion, and social resistance often generalise across communities, the person or organization in the central position, the information to diffuse, and the reason for resistance may and often does vary.
Typically, without a group-based intervention that forces the introduction of new information, most new information comes from outside sources (Granovetter 1973) such as mass media sources. If the baseline findings do not suggest that group-based interventions would be effective and programmers elect to produce mass media programmes, social network analysis may serve as a useful method to monitor mass media effects. Social marketing and entertainment-education strategies focus on mass media as a diffusion agent (Morris, 2003). Theories of two-step flow (Lazarfeld et al., 1944), social cognitive theory (Bandura 1997, 2004) and diffusion of innovations (Rogers, 2003) formalise the links between media programming and interpersonal communication. Media programmes spur interpersonal conversations, which then lead to the adoption of ideas, attitudes, or behaviours. In fact, one review suggests that peer networks play a critical role in the adoption of new ideas (Reardon & Rogers, 1988). A growing number of studies (e.g., Morris, 2003) gather information on these networks to design interventions and to monitor the efficacy of their media campaigns. Radios were ubiquitous in these catchments, and thus, radiobased entertainment-education may best reach the community, especially isolated members.
Network effects often work in tandem with entertainment-education. For example, researchers note that Twende na Wakati, the soap-opera campaign focusing on family planning in Tanzania, had strong effects because it stimulated conversations within social networks (Mohammed, 2001). Peer discussions about the programme showed statistically significant effects for increased family planning knowledge and contraceptive use, even after controlling for direct exposure to the programme. Interpersonal communication in social networks and mass media campaigns can yield unique and complementary positive effects.
Conclusion
This chapter has addressed how attention to community-level characteristics and social network analysis may be a useful tool for designing and evaluating HIV/AIDS interventions. Decision-making models using such information may promote prosocial community mobilisation and proactively avoid inequity, marginalisation, or discrimination. By identifying the social processes at the community level, we gained an understanding of how communities as a whole react and respond to HIV/AIDS, in order to better develop community-based health campaigns.
Acknowledgements
My thanks to Kim Witte, Erna Keulder, Research Facilitation Services (Windhoek, Namibia), Rajiv Rimal, JHUCCP/Namibia, Dan Morrison, and Lisa Murray-Johnson. This study was funded with primary support from the United States Agency for International Development under the Health Communication Partnership project (GPH-A-02-00008-00) based at Johns Hopkins/Bloomberg School of Public Health/Center for Communication Programmes. Most importantly, I am grateful to the citizens and leaders of Namibia for sharing their information with us.
References
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman.
Bandura, A. (2004). Health promotion by social cognitive means. Health Education & Behavior, 31, 143-164.
Borgatti, S.P., Everett, M.G., & Freeman, L.C. (2002). UCInet for Windows: Software for social network analysis. Harvard, MA: Analytic Technologies.
Cialdini, R.B. (2008). Influence: Science and practice (5th ed.). Boston, MA: Allyn & Bacon.
Cohen, J. (1994). The earth is round (p < .05). American Psychologist, 49, 997-1003.
Farquhar, J.W. (1978). The community-based model of life style intervention trials. American Journal of Epidemiology, 108, 103-111.
Figueroa, M.E., Kincaid, D.L., Rani, M., & Lewis, G. (2002). Communication for social change: An integrated model for measuring the process and its outcomes. Communication for Social Change Working Paper Series: No 1. New York, NY: Rockefeller Foundation.
Fishbein, M. (2000). The role of theory in HIV prevention. AIDS Care, 12, 273-278.
Fishbein, M., & Yzer, M.C. (2003). Using theory to design effective health behavior interventions. Communication Theory, 13, 164-183.
Fullilove, R.E., Green, L., & Fullilove, M.T. (2000). The Family to Family program: A structural intervention with implications for the prevention of HIV/AIDS and other community epidemics. AIDS, 14, S63-S67.
Gondolf, E.W. (2004). Evaluating batterer counseling programmes: A difficult task showing some effects and implications. Aggression and Violent Behavior, 9, 605-631.
Granovetter, M.S. (1973). The strength of weak ties. American Journal of Sociology, 78, 1360-1380.
Gruber, J., & Caffrey, M. (2005). HIV/AIDS and community conflict in Nigeria: Implications and challenges. Social Science & Medicine, 60, 1209-1218.
Keating, K., Love, R., Oliver, T., Peach, H., & Flynn, C. (1985). The Hood River Project: Take a walk on the applied side. The Rural Sociologist, 5, 112-118.
Kincaid, D.L. (2004). From innovation to social norm: Bounded normative influence. Journal of Health Communication, 9, 37-57.
Keulder, E., & Witte, K. (2003). In-depth interviews: The effect of culture and environment on the behaviour of Namibian youth. Baltimore, MD: Johns Hopkins University Center for Communication Programmes.
Lam, T.K., McPhee, S. J., Mock, J., Wong, C., Doan, H.T., Nguyen, T., Lai, K.Q., Ha-Ianconis, T., & Luong, T. (2003). Encouraging Vietnamese-American women to obtain pap tests through lay health worker outreach and media education. Journal of General Internal Medicine, 18, 516-524.
Lazarsfeld, P.F., Berelson, B., & Gaudet, H. (1944). The people’s choice. New York: Columbia University Press.
Makoul, G., & Roloff, M. (1998). The role of efficacy and outcome expectations in the decision to withhold relational complaints. Communication Research, 25, 5-29.
Mertens, F., Saint-Charles, J., Lucotte, M., & Mergler, D. (2008). Emergence and robustness of a community discussion network on Mercury contamination and health in the Brazilian Amazon. Health Education Behavior, 35, 509-521.
Mohammed, S. (2001). Personal communication networks and the effects of an entertainmenteducation radio soap opera in Tanzania. Journal of Health Communication, 6, 137-154.
Morris, N. (2003). A comparative analysis of the diffusion and participatory models in development communication. Communication Theory, 13, 225-248.
Mbuyazi, S.M. (2004). DramAidE: Participatory drama in South Africa. Democracy and Education, 23, 35-38.
Namibian Broadcasting Corporation. (2004). Namibian Broadcasting Corporation – Radio. Retrieved June 20, 2008 from http://www.nbc.com.na/radio/home.php.
Nutbeam, D., & Catford, J. (1987). The Welsh Heart Programme evaluation strategy: Progress, plans and possibilities. Health Promotion, 2, 5-18.
Pasick, R.J., Hiatt, R.A., & Paskett, E.D. (2004). Lessons learned from community-based cancer screening intervention research. Cancer, 101, 1146-1164.
Puska, P., Salonen, J.T., Tuomilehto, J., Nissinen, A., & Kottke, T.E. (1983). Evaluating community-based preventive cardiovascular programmes: Problems and experiences from the North Karelia Project. Journal of Community Health, 9, 49-64.
Putnam, R.D. (2000). Bowling alone: The collapse and revival of American community. New York: Touchstone.
Rodd, J., Gaskell, G., & Marslen-Wilson, W. (2000). The advantages and disadvantages of semantic ambiguity. Paper presented at the annual meeting of the Cognitive Science Society, Philadelphia, PA.
Rogers, E.M. (2003). Diffusion of innovations (5th ed.). New York: Free Press.
Ruiz-Casares, M. (2006). Strengthening the capacity of child-headed households in Namibia to meet their own needs: A social networks approach. Unpublished dissertation, Cornell University.
Smith, R.A., Ferrara, M., & Witte, K. (2007). Social sides of health risks: Stigma and collective efficacy in adopting AIDS orphans. Health Communication, 21, 1-10.
Smith, R.A., & Morrison, D. (2006). The impact of stigma, experience, and group referent on HIV risk assessments and HIV testing intentions in Namibia. Social Science & Medicine, 63, 2649-2660.
Smith, R.A., & Nguyen, L. (2008). Searching for a ‘generalized social agent’ to predict Namibians’ intentions to prevent sexual transmission of HIV. AIDS Care, 20, 242-250.
Smith, R.A., & Neidermyer, A. (in press). Keepers of the secret: Desires to conceal a family member’s HIV+ status in Namibia. Health Communication.
Smith, R.A., Witte, K., & Keulder, E. (2004). HIV/AIDS Strategic Information Report: Communities, group norms, and social change – A baseline social network analysis of residents from Andara, Nyangana, and Rundu (Wave 2, Round 1). Baltimore, MD: Johns Hopkins Bloomberg School of Public Health/Center for Communication Programmes.
Tjaronda, W. (May, 10, 2004). Red Cross day focuses on stigma. New Era. Retrieved September 4, 2007, from: http://www.newera.com.na/archives.php?id=1624&date=2004-05-10.
UNAIDS. (2002). Report on the global HIV/AIDS epidemic. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS).
UNAIDS. (2004). Report on the global AIDS epidemic. Geneva, Switzerland: Author.
UNAIDS. (2006). Report on the global AIDS epidemic. Geneva, Switzerland: Author.
U.S. Census Bureau. (2004). International Population Reports WP/02-2, The AIDS Pandemic in the 21st Century. Washington, DC: U.S. Government Printing Office.
Wasserman, S., & Faust. K. (1994). Social Network Analysis: Methods & applications. Cambridge, UK: Cambridge University Press.
Weenig, M.W.H., & Midden, C.J.H. (1991). Communication network influences on information diffusion and persuasion. Journal of Personality and Social Psychology, 61, 734-742.


You May Also Like



Comments
Leave a Reply

Search this site
About
Support
Follow us on Facebook & X & BlueSky
Archives
- December 2024
- November 2024
- October 2024
- September 2024
- August 2024
- July 2024
- June 2024
- May 2024
- April 2024
- March 2024
- February 2024
- January 2024
- December 2023
- November 2023
- October 2023
- September 2023
- August 2023
- July 2023
- June 2023
- May 2023
- April 2023
- March 2023
- February 2023
- January 2023
- December 2022
- November 2022
- October 2022
- September 2022
- August 2022
- July 2022
- June 2022
- May 2022
- April 2022
- March 2022
- February 2022
- January 2022
- December 2021
- November 2021
- October 2021
- September 2021
- August 2021
- July 2021
- June 2021
- May 2021
- April 2021
- March 2021
- February 2021
- January 2021
- December 2020
- November 2020
- October 2020
- September 2020
- August 2020
- July 2020
- June 2020
- May 2020
- April 2020
- March 2020
- February 2020
- January 2020
- December 2019
- November 2019
- October 2019
- September 2019
- August 2019
- July 2019
- June 2019
- May 2019
- April 2019
- March 2019
- February 2019
- January 2019
- December 2018
- November 2018
- October 2018
- September 2018
- August 2018
- July 2018
- June 2018
- May 2018
- April 2018
- March 2018
- February 2018
- January 2018
- December 2017
- November 2017
- October 2017
- September 2017
- August 2017
- July 2017
- June 2017
- May 2017
- April 2017
- March 2017
- February 2017
- January 2017
- December 2016
- November 2016
- October 2016
- September 2016
- August 2016
- July 2016
- June 2016
- May 2016
- April 2016
- March 2016
- February 2016
- January 2016
- December 2015
- November 2015
- October 2015
- September 2015
- August 2015
- July 2015
- June 2015
- May 2015
- April 2015
- March 2015
- February 2015
- January 2015
- December 2014
- November 2014
- October 2014
- September 2014
- August 2014
- July 2014
- June 2014
- May 2014
- April 2014
- March 2014
- February 2014
- January 2014
- December 2013
- November 2013
- October 2013
- September 2013
- August 2013
- July 2013
- June 2013
- May 2013
- April 2013
- March 2013
- February 2013
- January 2013
- December 2012
- November 2012
- October 2012
- September 2012
- August 2012
- July 2012
- June 2012
- May 2012
- April 2012
- March 2012
- February 2012
- January 2012
- December 2011
- November 2011
- October 2011
- September 2011
- July 2011
- June 2011
- May 2011
- April 2011
- March 2011
- February 2011
- January 2011